🗺️ What You Will Learn in This Article
- Describe the biochemical nature, synthesis site, and normal serum levels of AFP across the lifespan
- Explain why AFP is elevated in HCC, germ cell tumours, and other AFP-producing malignancies
- Interpret maternal serum AFP in the context of prenatal screening for NTDs and chromosomal anomalies
- Distinguish between causes of high vs low maternal AFP and link each to a specific diagnosis
- Use AFP as a monitoring tool in HCC treatment and surveillance
- Identify the specific clinical associations that generate NEET PG / USMLE MCQs on AFP every year
- Avoid the five most common mistakes students make about AFP in exams
📖 Introduction: Why AFP Matters in Exams
A 58-year-old man with known hepatitis B cirrhosis presents with a 3 kg weight loss, right upper quadrant pain, and a 4 cm hepatic mass on ultrasound. His serum AFP is 12,400 ng/mL. No biopsy is needed — this is hepatocellular carcinoma (HCC) diagnosed by imaging plus AFP criteria. AFP is one of the few tumour markers where a serum level alone, combined with imaging, meets diagnostic criteria without histology. That clinical weight — rare for any laboratory value — is why AFP appears in exams every year across biochemistry, pathology, and obstetrics simultaneously.
AFP intersects three major exam domains: oncology (HCC, germ cell tumours), obstetrics (maternal serum screening for NTDs and Down syndrome), and paediatrics (hepatoblastoma, yolk sac tumour, Ataxia-Telangiectasia). NEET PG regularly tests AFP in all three contexts. USMLE Step 1 often presents clinical vignettes where you must interpret a high or low AFP value in a pregnant woman or identify the tumour type from a serum AFP pattern. AIIMS tends to push deeper — asking about AFP isoforms (AFP-L3), the PIVKA-II co-marker, and the molecular biology of AFP gene expression.
This article covers AFP’s biochemistry, its normal levels across life stages, all clinically relevant causes of elevation and suppression, prenatal interpretation with cutoffs, and a full clinical monitoring framework for HCC. Every section is built around exam-ready facts.
🔬 AFP — Biochemistry & Normal Physiology
What Is AFP?
Alpha-fetoprotein (AFP) is a 70 kDa glycoprotein — the foetal analogue of albumin. It is encoded by the AFP gene on chromosome 4q13 and belongs to the albuminoid superfamily along with albumin and α-albumin (afamin). The protein is heavily glycosylated, and the pattern of glycosylation (lectin-binding isoforms) is clinically important for distinguishing benign from malignant causes of elevation.
Where and When Is AFP Synthesised?
AFP is produced sequentially by three sites during foetal development:
| Developmental Stage | Primary Synthesis Site | Serum Level |
|---|---|---|
| Early embryo (yolk sac stage) | Yolk sac | Very high |
| Foetal liver (dominant) | Hepatocytes | Peaks at ~3 mg/mL at 12–14 weeks gestation |
| Foetal GI tract | Gastrointestinal tract | Minor contribution |
| After birth | Synthesis rapidly shuts down | Falls to adult levels by 1 year |
| Adult (normal) | Trace hepatocyte expression | < 10–20 ng/mL |
The dramatic post-natal suppression of AFP synthesis is mediated by transcriptional repressors that silence the AFP gene in adult hepatocytes. Cancer cells reactivate this foetal gene — this is why elevated AFP in an adult is a red flag for malignancy.
AFP Isoforms — Lectin-Binding Subtypes
AFP glycoforms are separated by lectin affinity chromatography using Lens culinaris agglutinin (LCA):
| Isoform | Reactivity | Clinical Association |
|---|---|---|
| AFP-L1 | LCA non-reactive | Benign liver disease (cirrhosis, hepatitis) |
| AFP-L2 | LCA weakly reactive | Pregnancy (yolk sac origin) |
| AFP-L3 | LCA reactive | HCC-specific — used as cancer biomarker |
High-yield exam fact: AFP-L3 fraction ≥ 10–15% of total AFP strongly suggests HCC even when total AFP is only mildly elevated. AFP-L3 is the Japan-approved HCC biomarker and appears in AIIMS questions on advanced tumour markers.
📊 AFP Levels Across the Lifespan — Visual Reference
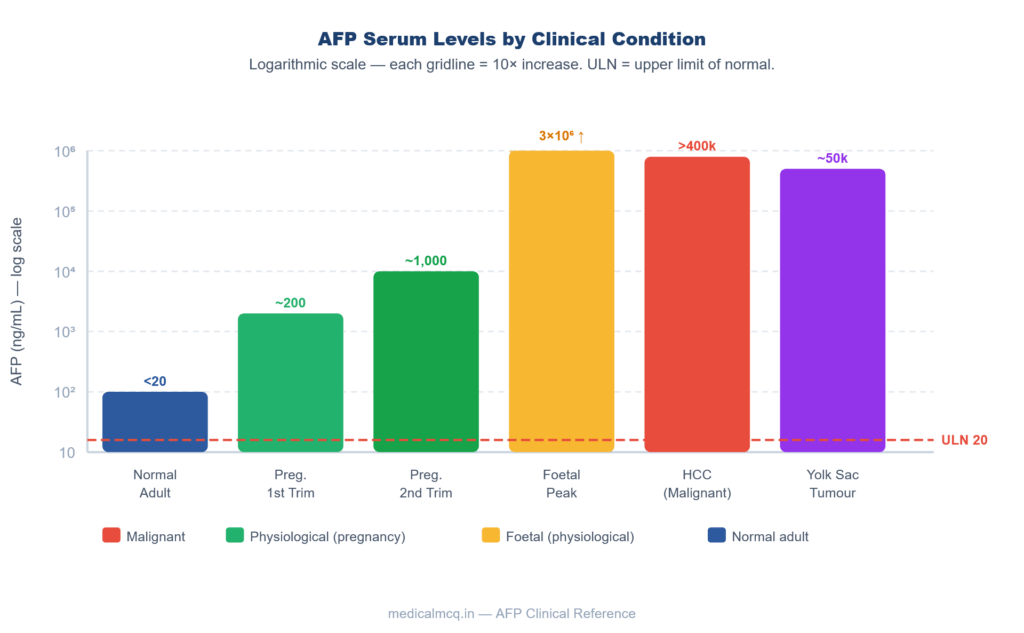
Fig 1 — AFP Serum Levels by Condition (Log₁₀ Scale)
Fig 1. AFP serum concentrations across clinical conditions plotted on a log₁₀ scale. Red dashed line = upper limit of normal (20 ng/mL) in adult non-pregnant individuals.
⚙️ AFP as a Tumour Marker — HCC & Germ Cell Tumours
Hepatocellular Carcinoma (HCC)
AFP is the primary serum tumour marker for HCC. In a patient with cirrhosis or chronic hepatitis B/C, a rising AFP signals possible HCC even before imaging detects a mass.
Diagnostic criteria (AASLD / EASL):
- AFP > 200 ng/mL in a high-risk patient (cirrhosis) with a compatible hepatic lesion on dynamic imaging = presumptive diagnosis of HCC (no biopsy required)
- AFP > 400 ng/mL historically considered highly specific for HCC
- AFP > 1,000 ng/mL — essentially diagnostic in the right clinical context
Important limitation: AFP is elevated in only 60–70% of HCC cases. AFP-negative HCC (30–40% of cases) requires imaging diagnosis. This is why AFP alone cannot be used as a screening test — it must be combined with liver ultrasound every 6 months in high-risk patients.
Causes of false-positive AFP elevation (benign):
| Benign Cause | Typical AFP Level | Distinguishing Feature |
|---|---|---|
| Liver regeneration (hepatitis flare) | 100–500 ng/mL | Transient, parallels liver enzymes |
| Cirrhosis (active) | Up to 200 ng/mL | Stable or slowly rising, no mass |
| Pregnancy | Up to 500 ng/mL | Clinical context obvious |
| Alcoholic hepatitis | Up to 100 ng/mL | Alcohol history, AST:ALT > 2:1 |
| Primary biliary cholangitis | Up to 50 ng/mL | ALP elevation, anti-mitochondrial Ab |
Germ Cell Tumours — AFP by Histology
AFP is produced by germ cell tumours containing yolk sac (endodermal sinus) elements. Pure seminomas do NOT produce AFP — this is a critical exam distinction.
| Tumour Type | AFP | β-hCG | Clinical Note |
|---|---|---|---|
| Yolk sac tumour (endodermal sinus) | ✅ Very HIGH | ❌ Negative | Most AFP-producing GCT |
| Mixed GCT (non-seminomatous) | ✅ High | ✅ Often high | Most common GCT in adults |
| Embryonal carcinoma | ✅ Mild–moderate | ✅ Variable | Aggressive; mixed patterns common |
| Choriocarcinoma | ❌ Negative | ✅ Very HIGH | Syncytiotrophoblast → β-hCG |
| Pure seminoma | ❌ NEVER elevated | ✅ Mildly elevated (10–20%) | AFP elevation = mixed, not pure seminoma |
| Mature teratoma | ❌ Negative | ❌ Negative | Benign; markers negative |
| Hepatoblastoma (paediatric) | ✅ Very HIGH | ❌ | Children < 5 years; AFP diagnostic |
🔴 Critical exam fact: A testicular mass with elevated AFP cannot be a pure seminoma — by definition. If AFP is elevated, there must be a non-seminomatous component. This changes staging and chemotherapy protocol.
AFP Monitoring in HCC Treatment
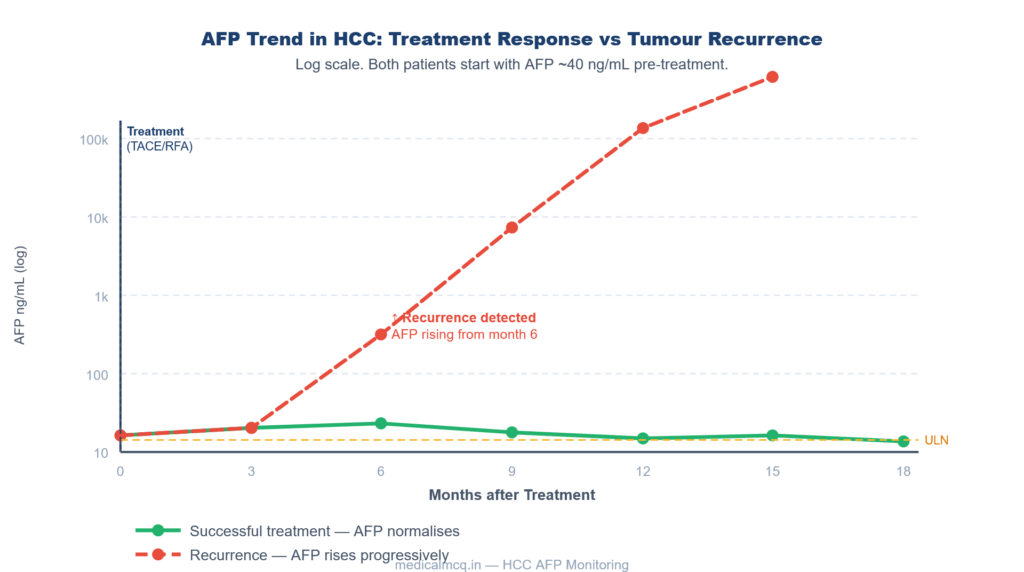
Fig 2 — AFP Monitoring in HCC: Treatment Response vs Recurrence
Fig 2. AFP monitoring after HCC treatment (TACE/RFA). Green = durable response (AFP stays at ULN). Red dashed = tumour recurrence (AFP rises from month 6). Rising AFP during surveillance = re-imaging urgently required.
🤰 AFP in Prenatal Screening
Maternal Serum AFP (MSAFP)
Maternal serum AFP (MSAFP) is measured at 15–20 weeks gestation (ideally 16–18 weeks). Results are reported as Multiples of the Median (MoM) adjusted for:
- Gestational age
- Maternal weight
- Ethnicity
- Presence of diabetes
- Number of foetuses
Normal MSAFP: 0.5–2.5 MoM
High MSAFP (> 2.5 MoM) — Causes
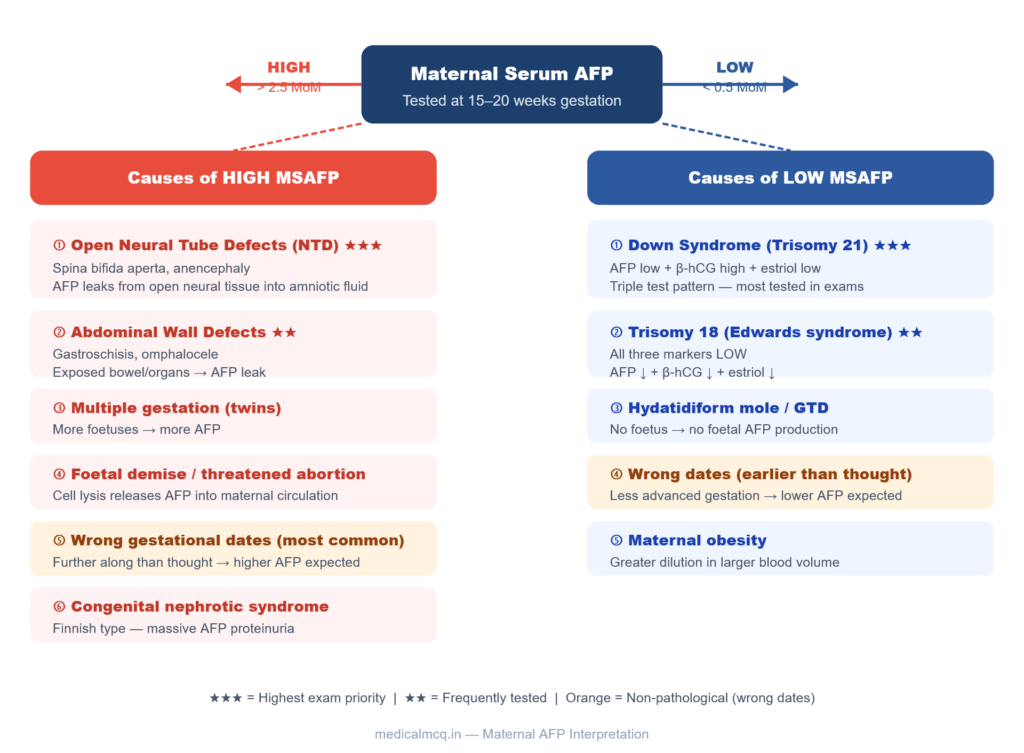
Fig 3 — Maternal Serum AFP Interpretation Guide
Maternal Serum AFP Tested at 15–20 weeks gestation HIGH > 2.5 MoM LOW < 0.5 MoM Causes of HIGH MSAFP ① Open Neural Tube Defects (NTD)
★★★ Spina bifida aperta, anencephaly AFP leaks from open neural tissue into amniotic fluid ② Abdominal Wall Defects
★★ Gastroschisis, omphalocele Exposed bowel/organs → AFP leak ③ Multiple gestation (twins) More foetuses → more AFP ④ Foetal demise / threatened abortion Cell lysis releases AFP into maternal circulation ⑤ Wrong gestational dates (most common) Further along than thought → higher AFP expected ⑥ Congenital nephrotic syndrome Finnish type — massive AFP proteinuria Causes of LOW MSAFP ① Down Syndrome (Trisomy 21)
★★★ AFP low + β-hCG high + estriol low Triple test pattern — most tested in exams ② Trisomy 18 (Edwards syndrome)
★★ All three markers LOW AFP ↓ + β-hCG ↓ + estriol ↓ ③ Hydatidiform mole / GTD No foetus → no foetal AFP production ④ Wrong dates (earlier than thought) Less advanced gestation → lower AFP expected ⑤ Maternal obesity Greater dilution in larger blood volume
Fig 3. Maternal serum AFP interpretation at 15–20 weeks. High AFP (left) → mainly structural defects. Low AFP (right) → chromosomal anomalies. Wrong gestational dates (orange) is the most common non-pathological cause of both high and low readings.
The Triple Test and Quad Screen
The Triple Test (second trimester, 15–20 weeks) measures:
| Marker | Down Syndrome (T21) | Edwards (T18) | Open NTD |
|---|---|---|---|
| MSAFP | ↓ Low | ↓ Low | ↑↑ High |
| β-hCG | ↑ High | ↓ Low | Normal |
| Unconjugated estriol (uE3) | ↓ Low | ↓ Low | Normal |
The Quad Screen adds inhibin-A (elevated in Down syndrome) to the triple test, improving sensitivity to ~80% for trisomy 21.
🟠 Exam mnemonic for Down syndrome triple test: “DOwN — Down is only uNusual”
AFP ↓ + β-hCG ↑ + estriol ↓ = Trisomy 21. The ONE marker going UP is β-hCG. Everything else is down.
🏥 AFP in Special Clinical Contexts
AFP in Ataxia-Telangiectasia (A-T)
One of the most tested AFP facts in NEET PG and USMLE is that serum AFP is persistently elevated in Ataxia-Telangiectasia — a non-malignant cause of elevated AFP in children. The mechanism: defective ATM kinase → impaired hepatic maturation → failure to fully suppress foetal AFP gene expression postnatally.
Clinical picture: Cerebellar ataxia + oculocutaneous telangiectasias + immunodeficiency + elevated AFP (> 10 ng/mL, often > 100 ng/mL) + normal β-hCG + no hepatic mass.
This is the most important non-malignant, non-pregnant cause of elevated AFP in a child to memorise.
AFP in Hepatoblastoma
Hepatoblastoma is the most common liver tumour in children under 5 years. AFP is markedly elevated (often > 100,000 ng/mL) and is used for:
- Initial diagnosis (combined with imaging)
- Surgical resection planning (AFP guides operability assessment)
- Post-treatment monitoring (falling AFP = response; rising = recurrence)
AFP is so reliably elevated in hepatoblastoma that a normal AFP in a child with a liver mass should raise doubt about the diagnosis.
AFP and Liver Regeneration
AFP rises transiently during liver regeneration — after hepatitis flares, post-hepatectomy, and during treatment of hepatitis B/C. This rise is benign and must be distinguished from HCC:
- Regeneration AFP: usually < 200 ng/mL, parallels ALT/AST, falls as hepatitis resolves
- HCC AFP: typically > 400 ng/mL, rises progressively, associated with a mass on imaging
🔄 How AFP Connects to Other Topics
- → Liver Disease — Cirrhosis is the strongest risk factor for HCC → AFP monitoring every 6 months with ultrasound is standard of care in Child-Pugh A/B cirrhosis.
- → Germ Cell Tumours — AFP + β-hCG together are the backbone of testicular GCT staging and treatment monitoring. IGCCCG risk stratification uses both markers.
- → Prenatal Diagnosis — MSAFP is the entry point into a cascade of investigations including amniocentesis (for amniotic fluid AFP + AChE in NTD), detailed anomaly ultrasound, and karyotyping.
- → Oncology — PARP Inhibitors — AFP-producing HCC in BRCA-mutant patients may be candidates for novel combination therapy trials; the DNA repair / HCC connection links two major biochemistry topics.
- → Immunology — A-T — AFP elevation is a laboratory criterion for diagnosing Ataxia-Telangiectasia alongside IgA deficiency, low lymphocyte count, and chromosomal fragility.
- → Pharmacology — Sorafenib (first-line systemic therapy for HCC) reduces AFP in responders. AFP response predicts radiological response and survival — connecting pharmacology to tumour marker interpretation.
🎯 High-Yield Exam Facts
🔴 AFP is the foetal analogue of albumin — not a foetal immunoglobulin or hormone
Synthesised by yolk sac → foetal hepatocytes → GI tract. Peaks at 12–14 weeks of gestation at ~3 mg/mL. Suppressed postnatally; normal adult level < 20 ng/mL.
🔴 Pure seminoma NEVER produces AFP — AFP elevation = non-seminomatous component
If AFP is elevated in a testicular mass, it cannot be a pure seminoma regardless of the histology report. This changes staging, surgical approach, and chemotherapy.
🔴 Open NTDs cause HIGH MSAFP; Down syndrome causes LOW MSAFP
This directional pair is the single most-tested AFP fact in NEET PG obstetrics. Open (not closed) NTDs allow AFP to leak. Closed NTDs (e.g. spina bifida occulta) do NOT raise MSAFP.
🔴 AFP is elevated in Ataxia-Telangiectasia — a non-malignant cause in children
Due to impaired postnatal AFP suppression from ATM deficiency. Paired with ataxia + telangiectasia + elevated serum AFP = diagnostic for A-T.
🟠 AFP-L3 isoform ≥ 10–15% is specific for HCC regardless of total AFP level
AFP-L3 is produced only by malignant hepatocytes, not by regenerating normal hepatocytes. Used in Japan as an approved HCC biomarker alongside PIVKA-II (des-gamma-carboxyprothrombin).
🟠 Triple test for Down syndrome: AFP ↓ + β-hCG ↑ + estriol ↓
For Edwards syndrome (T18): all three markers are LOW. This distinction is directly tested in NEET PG and FMGE.
🟠 Wrong gestational dates is the most common cause of abnormal MSAFP
Always correct for gestational age first before interpreting any MSAFP result. Dates that are off by even 1–2 weeks shift the MoM significantly.
🟠 AFP monitoring in HCC: fall after treatment = response; rise = recurrence
A rising AFP during surveillance warrants immediate reimaging even if the AFP level is still below the diagnostic cutoff.
🟡 Congenital nephrotic syndrome (Finnish type) causes HIGH MSAFP — not low
Often confused with Down syndrome. Congenital nephrotic syndrome → massive proteinuria → AFP leaks into amniotic fluid and maternal serum → MSAFP is HIGH, not low.
🟡 AFP does NOT cross-react with β-hCG and vice versa — they are entirely separate proteins
Some students confuse AFP with β-hCG as both are raised in GCTs. They are structurally unrelated and produced by different tumour components.
🟡 Hepatoblastoma AFP > 100,000 ng/mL is common; a normal AFP in a child with a liver mass should question the diagnosis
The exception: small cell undifferentiated hepatoblastoma (anaplastic) may have low AFP — this variant carries the worst prognosis.
🧠 Mnemonics & Memory Tricks
Mnemonic 1 — Triple Test for Down Syndrome
“DOWN — One UP, rest Down”
- AFP → Down
- β-hCG → Over (the only one that goes UP)
- Estriol → Weak (down)
- Not normal
💡 Exam trigger: Any question asking “which triple test pattern suggests Down syndrome?” — the key is β-hCG is elevated while the other two are low.
Mnemonic 2 — Causes of High MSAFP
“NOMADS Have Fat Abdomen”
| Letter | Cause |
|---|---|
| N | Neural tube defects (open) |
| O | Omphalocele / gastroschisis (abdominal wall defects) |
| M | Multiple gestation (twins) |
| A | Abruptio placentae / foetal demise |
| D | Dates wrong (gestational age miscalculation) |
| H | Hepatic — maternal liver disease |
| F | Finnish nephrotic syndrome |
| A | Abdominal wall defects (catches the remaining ones) |
💡 Learn the first 5 — they cover 95% of exam questions on high MSAFP.
Mnemonic 3 — AFP-Producing Tumours
“HCC Yells Enough” → H-Y-E
- H — Hepatocellular Carcinoma
- Y — Yolk Sac Tumour (endodermal sinus)
- E — Embryonal carcinoma (mixed GCT)
💡 Exam trigger: “Which tumour markers are elevated in non-seminomatous GCT?” → AFP (yolk sac/embryonal) + β-hCG (choriocarcinoma component).
⚠️ Common Mistakes Students Make on AFP
❌ Mistake: “Closed spina bifida (spina bifida occulta) raises MSAFP”
✅ Reality: Only open NTDs raise MSAFP. In closed NTDs, the neural tissue is covered by skin → AFP cannot leak. MSAFP is normal.
📝 How it’s tested: “A pregnant woman at 17 weeks has MSAFP 3.8 MoM. Ultrasound shows a skin-covered lumbar defect. Explain the AFP result.” — The AFP finding would NOT be explained by a closed defect. Look for a second explanation.
❌ Mistake: “AFP is elevated in all testicular tumours”
✅ Reality: Pure seminoma → AFP is always normal. AFP elevation in any testicular mass by definition excludes pure seminoma.
📝 How it’s tested: “Orchidectomy specimen shows pure seminoma on histology but preoperative AFP was 4200 ng/mL — what is the correct interpretation?” — The correct answer: the tumour cannot be purely seminomatous; there must be a non-seminomatous component missed on sampling.
❌ Mistake: “Normal AFP excludes HCC”
✅ Reality: AFP is elevated in only 60–70% of HCC cases. AFP-negative HCC occurs in 30–40% of patients. AFP alone cannot rule out HCC — imaging (triphasic CT / MRI with arterial enhancement + washout) is essential.
📝 How it’s tested: “A cirrhotic patient has a 3 cm hepatic mass with arterial enhancement and washout on MRI but AFP is 8 ng/mL. Should HCC be excluded?” — No. Imaging criteria alone are sufficient for HCC diagnosis per AASLD guidelines.
❌ Mistake: “All three triple test markers are elevated in Down syndrome”
✅ Reality: In Down syndrome — AFP ↓ and estriol ↓, but β-hCG ↑. All three are elevated only if you confuse it with a different condition.
📝 How it’s tested: Listed in a table as a matching question — “Match the triple test pattern to the diagnosis.” Edwards syndrome (T18) is the one where ALL THREE are low.
❌ Mistake: “AFP elevation in A-T (Ataxia-Telangiectasia) means the child has cancer”
✅ Reality: AFP is chronically elevated in A-T due to defective ATM-dependent hepatic maturation — it is NOT a sign of malignancy. However, A-T patients DO have elevated cancer risk (lymphoma, leukaemia). The AFP elevation itself is a diagnostic criterion for A-T, not a cancer marker in this context.
📝 How it’s tested: Vignette of child with progressive ataxia + telangiectasias + elevated AFP. Options include “HCC” and “Ataxia-Telangiectasia.” The AFP here is a feature of A-T, not evidence of a liver tumour.
📝 5 Practice MCQs — Test Yourself Now
Q1 — Pure Recall (Easy)
The primary site of AFP synthesis in the developing embryo before hepatic organogenesis is complete is:
- A. Placental trophoblasts
- B. Foetal bone marrow
- C. Yolk sac
- D. Foetal adrenal cortex
👉 Click to reveal answer
Q2 — Pattern Recognition (Easy–Medium)
A 17-week pregnant woman undergoes triple screening. Results: MSAFP 0.4 MoM, β-hCG 2.8 MoM, unconjugated estriol 0.5 MoM. Which diagnosis is most consistent with this pattern?
- A. Open spina bifida
- B. Trisomy 21 (Down syndrome)
- C. Trisomy 18 (Edwards syndrome)
- D. Gastroschisis
👉 Click to reveal answer
Q3 — Application (Medium)
A 34-year-old man undergoes right orchidectomy for a 3.5 cm testicular mass. Pre-operative tumour markers: AFP 3,800 ng/mL, β-hCG 45 IU/L, LDH elevated. Histology of the orchidectomy specimen reports “pure classical seminoma.” What is the correct management conclusion?
- A. Treat as pure seminoma — AFP may be mildly elevated in seminoma
- B. The pathology report is likely incorrect; re-examine specimen for non-seminomatous elements
- C. The AFP elevation is from concurrent liver disease; proceed with seminoma protocol
- D. AFP > 1,000 ng/mL always indicates seminoma recurrence
👉 Click to reveal answer
Q4 — Clinical Scenario (Medium–Hard)
A 6-year-old boy presents with progressive gait ataxia, bilateral conjunctival telangiectasias, and recurrent respiratory infections. Serum AFP is 142 ng/mL. Liver ultrasound shows no mass. IgA is undetectable. Which of the following best explains the elevated AFP?
- A. Hepatocellular carcinoma arising on a background of chronic hepatitis
- B. Yolk sac tumour of the posterior fossa
- C. Impaired postnatal AFP gene suppression due to ATM kinase deficiency
- D. Maternal AFP crossing the placenta and persisting in the child
👉 Click to reveal answer
Q5 — Integration (Hard)
A 52-year-old man with Child-Pugh B hepatitis C cirrhosis has been on 6-monthly HCC surveillance. His AFP trend over 18 months: 18 → 22 → 28 → 65 → 180 → 520 ng/mL. Liver ultrasound at month 18 shows a 2.2 cm arterially enhancing nodule with washout on portal phase. What is the most appropriate next step and what does the AFP trend indicate?
- A. Repeat AFP in 3 months; the trend is within normal variation for cirrhosis
- B. Proceed to diagnostic liver biopsy before any treatment decision
- C. The AFP trend indicates HCC recurrence after previous treatment
- D. Diagnose HCC based on imaging criteria; AFP trend confirms ongoing tumour activity — initiate treatment without biopsy
👉 Click to reveal answer
📚 References
- 📖 Harrison’s Principles of Internal Medicine — Kasper et al. | Chapter 78: Liver Tumours; Chapter 82: Testicular Cancer
- 📖 Robbins Basic Pathology — Kumar, Abbas et al. | Chapter 15: Liver and Biliary Tract; Chapter 17: Male Genital System
- 📖 Williams Obstetrics — Cunningham et al. | Chapter 14: Prenatal Diagnosis
- 📖 Harper’s Illustrated Biochemistry — Murray, Rodwell et al. | Chapter on Plasma Proteins
- 📖 Lippincott’s Illustrated Reviews: Biochemistry — Ferrier | Chapter on Plasma Proteins and Tumour Markers
- 📖 AASLD Practice Guidance on HCC (2018) — Marrero JA et al. | Hepatology 68(2):723–750
🚀 Keep Practising — You Are Not Done Yet
AFP appears across Biochemistry, Pathology, and Obstetrics in NEET PG — sometimes in the same paper, in different departments. The theory you have read is your foundation. Applying it under timed pressure is what converts that foundation into marks.
medicalmcq.in has free MCQs across all three subjects — every one with a detailed explanation exactly like the answers above.